Malaria and Dengue — Global Case Study
Malaria kills a child every two minutes. Not because we lack the knowledge to prevent it — we have bed nets, insecticides, antimalarial drugs, and a working vaccine. It persists because of poverty, geography, and the relentless pressure of natural selection on both the parasite and the mosquito.
Practise this lesson
Four printable worksheets that build from the foundations up to exam-style questions — start at whatever level suits you.
Malaria kills more people annually than any armed conflict currently ongoing. Yet it is both preventable and treatable. Dengue infects 390 million people per year — four times more than malaria — yet has only recently had a partially effective vaccine approved.
Before reading: why do you think diseases like malaria and dengue persist despite decades of effort to control them? Predict at least three reasons — biological, social, or economic.
Know
- The causative agents, vectors, and transmission of malaria and dengue
- The global distribution and burden of each disease
- The main control strategies used for each disease
- Why control of these diseases remains difficult
Understand
- How the Plasmodium life cycle creates multiple intervention points
- Why drug resistance in malaria is such a significant problem
- Why dengue is harder to vaccinate against than malaria
Can Do
- Analyse data on disease burden and control effectiveness
- Evaluate multiple control strategies for a vector-borne disease
- Apply knowledge from L14–L17 to a real disease case study
Core Content
A eukaryotic parasite with a life cycle full of intervention points
Malaria is caused by Plasmodium parasites — single-celled eukaryotes (not bacteria or viruses) transmitted by infected female Anopheles mosquitoes. Five species infect humans; P. falciparum causes the most severe and lethal form.
In 2022, there were an estimated 249 million malaria cases globally, causing approximately 608,000 deaths — 76% of which were children under five. Sub-Saharan Africa bears approximately 95% of the global malaria burden.
The Plasmodium Life Cycle — Multiple Intervention Points
Each life cycle stage offers a different intervention point — vector control (mosquito), vaccines (liver stage), drugs (blood stage)
Control Strategies for Malaria
| Strategy | Mechanism | Effectiveness | Limitations |
|---|---|---|---|
| Insecticide-treated bed nets (ITNs) | Pyrethroid kills mosquitoes contacting net; physical barrier prevents bites during sleep | ~50–60% reduction in child malaria mortality in high-use areas | Pyrethroid resistance growing; must be used consistently; periodic re-treatment needed |
| Indoor residual spraying (IRS) | Insecticide sprayed on interior walls kills resting mosquitoes | Very effective in targeted programs; contributed to historic reductions | Insecticide resistance; community acceptance; logistical complexity |
| Artemisinin combination therapy (ACT) | Rapidly kills blood-stage parasites | Gold-standard treatment; highly effective when taken correctly | Artemisinin partial resistance emerging in Southeast Asia and Africa |
| RTS,S vaccine (Mosquirix) | Targets sporozoite surface protein — blocks liver-stage invasion | ~36% efficacy against clinical malaria in young children | Requires 4-dose schedule; waning immunity; modest efficacy |
| R21/Matrix-M vaccine | Next-generation vaccine — higher antigen density than RTS,S | ~75–80% efficacy in trials; WHO approved 2023 — most effective malaria vaccine to date | Still requires booster; scale-up ongoing |
What to write in your book
- Malaria = Plasmodium (eukaryotic parasite), vector = female Anopheles; P. falciparum most lethal.
- 608,000 deaths/year, 95% in sub-Saharan Africa, 76% children under 5.
- Life cycle: mosquito → liver (asymptomatic) → blood (fever) — each stage is an intervention point.
- Control: ITNs, IRS, ACT drugs, RTS,S (36%) and R21 (75–80%) vaccines.
Malaria is caused by _____, a single-celled eukaryotic parasite transmitted by female Anopheles mosquitoes.

Plasmodium Life Cycle
Four serotypes, antibody-dependent enhancement, and a vaccine paradox
Dengue fever is caused by dengue virus (DENV), a flavivirus with four distinct serotypes (DENV-1, 2, 3, 4). It is transmitted by Aedes aegypti mosquitoes — urban mosquitoes that breed in small water containers and bite during the day. Dengue infects an estimated 390 million people per year; approximately 96 million develop clinical illness and around 20,000 die. It is endemic in over 100 countries and cases have increased eightfold since 2000.
Why Dengue Is Especially Difficult to Vaccinate Against
Infection with one dengue serotype provides lifelong immunity to that serotype but only short-term cross-protection against the others. A second infection with a different serotype can cause antibody-dependent enhancement (ADE) — pre-existing antibodies from the first infection facilitate entry of the second serotype into immune cells, amplifying the infection. This causes severe dengue (dengue haemorrhagic fever), which can be fatal.
A dengue vaccine must therefore provide strong, balanced, long-lasting immunity against all four serotypes simultaneously. If it protects well against only some serotypes, vaccinated individuals could be immunologically primed for ADE — worse off than if unvaccinated.
Control Strategies for Dengue
Vector control (breeding sites)
Wolbachia release
GM mosquitoes (OX513A)
TAK-003 vaccine (Qdenga)
What to write in your book
- Dengue = DENV virus, 4 serotypes; vector = Aedes aegypti (daytime, urban).
- One infection = lifelong immunity to THAT serotype only; second serotype can trigger ADE → severe dengue.
- A vaccine must protect against all four serotypes equally or it can prime ADE (Dengvaxia harm in seronegatives).
- Control: remove breeding water, Wolbachia release, GM mosquitoes, TAK-003 vaccine.
Why can a second dengue infection with a different serotype be more dangerous than the first?
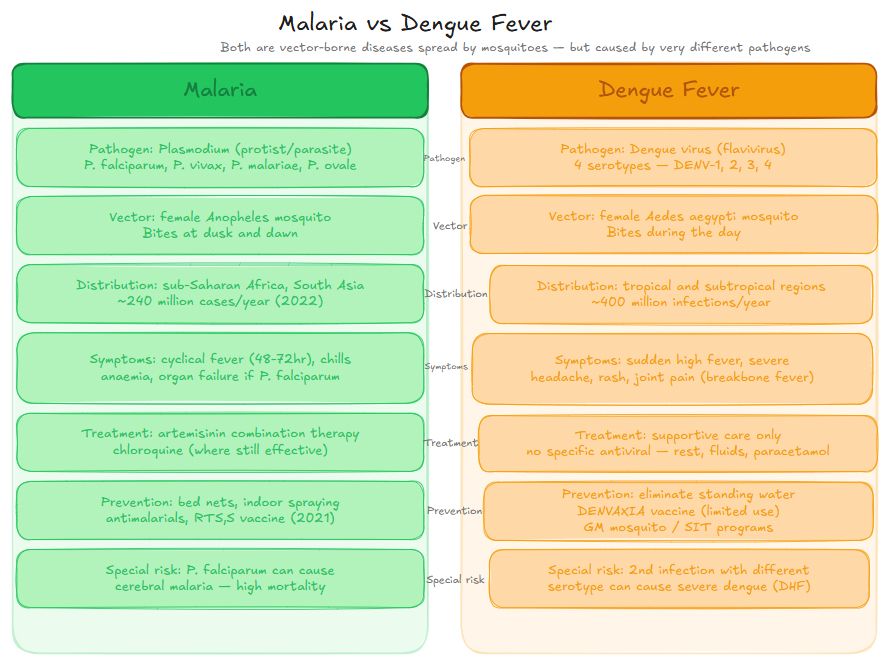
Malaria vs Dengue Comparison
Same delivery method, completely different biology
Malaria
- Pathogen: Plasmodium spp. (eukaryotic parasite)
- Vector: Female Anopheles (nocturnal biter)
- Immunity: Partial, acquired — not sterilising
- Treatment: ACT effective; resistance emerging
- Vaccine: RTS,S (36%) and R21 (75–80%)
- Distribution: Sub-Saharan Africa (95% of cases)
- Deaths: ~608,000/year; 76% children under 5
Dengue
- Pathogen: DENV virus — 4 serotypes (RNA flavivirus)
- Vector: Aedes aegypti (daytime biter; urban)
- Immunity: Lifelong to one serotype; ADE risk on second
- Treatment: No specific antiviral — supportive care only
- Vaccine: TAK-003 (partial); Dengvaxia (seropositive only)
- Distribution: Tropical Asia, Americas, expanding globally
- Infections: ~390 million/year; ~20,000 deaths
What to write in your book
- Malaria: Plasmodium parasite, Anopheles (night), ACT + R21 vaccine, 608k deaths/year.
- Dengue: DENV virus (4 serotypes), Aedes aegypti (day, urban), no specific antiviral, ~20k deaths/year.
- Both vector-borne but biologically very different — different pathogen, vector, immunity, and treatment.
Malaria and dengue are caused by the same type of pathogen.
The Plasmodium parasite has a complex life cycle involving both human and mosquito hosts.
Dengue fever is transmitted by Anopheles mosquitoes, the same vector that transmits malaria.
Error Spotting — Malaria and Dengue
Pattern B — Error Spotting
A student wrote the following passage about malaria and dengue. It contains four factual errors. Identify each, explain what is wrong, and write the correction.
- List the four errors in the passage.
- For each error, write one sentence explaining what is wrong and the correct information.
- Rewrite the passage correctly in your own words.
In 2022, malaria killed approximately 608,000 people. Roughly 76% were children under five. The arithmetic is blunt: one child every two minutes, around the clock, every day of the year.
You will analyse control strategy data in Activity 1 and evaluate these diseases in Short Answer Q3.
Malaria — Key Facts
- Pathogen: Plasmodium spp. (eukaryote); P. falciparum most lethal.
- Vector: female Anopheles (nocturnal).
- 608,000 deaths/year; 95% sub-Saharan Africa; 76% children under 5.
- Control: ITNs, IRS, ACT drugs, R21 vaccine (75–80% efficacy).
Dengue — Key Facts
- Pathogen: DENV virus, 4 serotypes — one infection does not protect against others.
- Vector: Aedes aegypti (daytime; urban).
- 390 million infections/year; ~20,000 deaths.
- ADE: second serotype infection can be more severe due to enhancing antibodies.
Why Control Is Difficult
- Drug and insecticide resistance (natural selection).
- No sterilising immunity (partial or serotype-specific).
- Remote areas, limited healthcare infrastructure.
- Climate change expanding vector ranges.
- Funding gaps in high-burden, low-income countries.
Plasmodium Life Cycle
- Mosquito stage → infected bite → liver stage (asymptomatic) → blood stage (fever, symptoms).
- Liver: primaquine + RTS,S/R21 vaccine targets sporozoites.
- Blood: ACT drugs kill merozoites in RBCs.
- Mosquito: ITNs, IRS, SIT eliminate vector.
Malaria and Dengue — Global Burden
A fresh set drawn from this lesson's question bank — feedback shown immediately. +5 XP per correct · +25 XP all correct
Pick your answer, then rate your confidence — that tells the system what to drill next.
ApplyBand 4(3 marks) 1. Describe the life cycle of Plasmodium falciparum, identifying at least three stages and explaining how each creates an opportunity for disease control.
1 mark per stage correctly identified with intervention opportunity (max 3): mosquito + vector control; liver + primaquine/RTS,S/R21; blood + ACT
UnderstandBand 4(3 marks) 2. Explain why dengue is more difficult to vaccinate against than malaria. Refer to the number of serotypes, antibody-dependent enhancement, and the Dengvaxia program.
1 mark: 4 serotypes — balanced protection required · 1 mark: ADE mechanism — partial protection creates severe dengue risk · 1 mark: Dengvaxia harm in seronegative individuals — program halted
EvaluateBand 5(4 marks) 3. Evaluate the effectiveness of integrated malaria control in sub-Saharan Africa between 2000 and 2022. Describe evidence of success, explain why progress has stalled since 2015, and assess the potential impact of the R21 vaccine.
1 mark: success evidence with specific data (deaths 121→51 per 100,000; case reduction) · 1 mark: reasons for stall (ITN plateau, resistance, COVID-19) · 1 mark: R21 potential at scale · 1 mark: overall evaluative conclusion
Show all answers
Multiple choice
Q1 — B: Plasmodium is a eukaryotic parasite — antibiotics target bacterial cell walls and ribosomes (absent in Plasmodium); antivirals target viral replication machinery (Plasmodium is not a virus). Specific antimalarial drugs target parasite-unique processes. (C) is wrong — Plasmodium does express surface antigens; vaccines targeting them are now approved. (D) is wrong — malaria always requires the mosquito vector.
Q2 — C: The liver stage is asymptomatic, creating an important window to eliminate parasites before illness begins. Primaquine kills liver-stage parasites; RTS,S/R21 vaccines block sporozoite invasion of liver cells. (A) is wrong — symptoms occur in the blood stage. (B) is wrong — sexual reproduction occurs in the mosquito gut, not the liver.
Q3 — D: ADE occurs when pre-existing antibodies from a first serotype bind but cannot neutralise the second serotype — instead facilitating its entry into Fc receptor-bearing immune cells, dramatically amplifying infection. (A) is the opposite of ADE. (B) describes a different evasion mechanism. (C) is incorrect.
Q4 — A: ITNs work via physical barrier (prevents bites during sleep) and pyrethroid coating (kills mosquitoes landing on the net). (B), (C), and (D) are all biologically incorrect descriptions of how ITNs function.
Q5 — C: Wolbachia does not kill mosquitoes — it reduces their vector competence (ability to transmit dengue). No lethal selection pressure means there is no mechanism for insecticide-style resistance to evolve. (A) is wrong — mosquito population is maintained. (B) is wrong — Wolbachia competes intracellularly with the virus, not via a toxin. (D) misunderstands the mechanism.
Short Answer Model Answers
SA1: The Plasmodium falciparum life cycle alternates between mosquito and human hosts. Stage 1 — the mosquito stage: sporozoites develop in the mosquito's salivary glands after sexual reproduction in the mosquito gut. This stage is targeted by vector control — insecticide-treated bed nets and indoor residual spraying kill or repel Anopheles mosquitoes before they can deliver sporozoites in an infected bite. Stage 2 — the liver stage: sporozoites injected during a bite rapidly migrate to the liver, invading hepatocytes and multiplying asexually to produce thousands of merozoites. No symptoms occur. The drug primaquine kills liver-stage parasites. The RTS,S and R21 vaccines block sporozoite invasion of liver cells by stimulating antibodies against the circumsporozoite protein — eliminating parasites before the symptomatic blood stage begins. Stage 3 — the blood stage: merozoites released from the liver invade red blood cells, multiply, rupture the cells (causing the characteristic fever and anaemia of malaria), and release more merozoites. ACT (artemisinin combination therapy) kills blood-stage parasites rapidly, treating illness and reducing transmission by limiting gametocyte production.
SA2: Dengue is more difficult to vaccinate against than malaria for three interconnected reasons. First, dengue virus has four antigenically distinct serotypes (DENV-1, 2, 3, 4). A vaccine must provide strong, balanced, lasting immunity against all four simultaneously — a far more complex immunological target than the relatively stable sporozoite protein targeted by the malaria vaccines. Second, the phenomenon of antibody-dependent enhancement (ADE) creates a paradoxical risk. If a vaccine provides immunity against some serotypes but not others, vaccinated individuals may be worse off than unvaccinated — pre-existing antibodies from the vaccine-induced response can facilitate entry of unprotected serotypes into Fc receptor-bearing immune cells, amplifying the infection and potentially causing severe dengue haemorrhagic fever. Third, the Dengvaxia program in the Philippines demonstrated this risk in practice. Given to over 800,000 schoolchildren in 2016, including many who had never previously had dengue (seronegative), subsequent analysis showed seronegative recipients were at higher risk of severe dengue after vaccination — exactly the ADE effect. The program was halted, criminal investigations were launched, and Dengvaxia is now recommended only for seropositive individuals — the opposite of the original target population.
SA3: Between 2000 and 2015, integrated malaria control programs in sub-Saharan Africa achieved substantial progress. Malaria deaths per 100,000 fell from 121 to 51 — a reduction of approximately 58% — as insecticide-treated bed net coverage increased from 2% to 65% of households and ACT became widely available. Case numbers also fell from ~370 to ~218 per 100,000. This represented millions of lives saved and one of global health's most significant achievements in the early 21st century. Since 2015, however, progress has stalled. Death rates stabilised in the 51–62 range rather than continuing to decline. ITN coverage plateaued at approximately 62–65% of households — logistical, funding, and population growth constraints appear to have limited further scale-up. Pyrethroid resistance in Anopheles populations is progressively reducing the killing effectiveness of treated nets in many areas. Artemisinin partial resistance, first detected in Southeast Asia, is increasingly found in African P. falciparum populations, threatening the gold-standard treatment. The COVID-19 pandemic in 2020 severely disrupted malaria service delivery — the data show a notable spike in both cases (238 per 100,000) and deaths (62 per 100,000) in that year, despite ACT nominally remaining available. The R21/Matrix-M vaccine, with approximately 75–80% efficacy approved by the WHO in 2023, has the potential to significantly accelerate malaria control beyond what bed nets and drugs alone can achieve. If deployed at scale — particularly to children under five, who bear 76% of malaria deaths — it could drive substantial further reductions in mortality even in areas where insecticide and drug resistance is limiting existing tools. Cold chain requirements, healthcare system capacity, and sustained funding remain constraints on deployment. Overall, the 2000–2015 period demonstrates what sustained, scaled investment in integrated malaria control can achieve. The post-2015 stall is a serious warning: without new tools, continued investment, and strategies to address resistance, the gains of the previous decade risk being eroded by biology and demography.
Five timed questions on malaria, dengue, and global disease control. Beat the boss to bank a tier — gold (perfect + fast), silver (80%+), or bronze (cleared).
⚔ Enter the arenaDefend your ship by blasting the correct answers for Malaria and Dengue — Global Case Study. Scores count toward the Asteroid Blaster leaderboard.
☄️ Play Asteroid Blaster →You were asked to predict why malaria and dengue persist despite decades of control effort.
The biological reasons: drug and insecticide resistance (natural selection making tools progressively less effective); complex multi-stage life cycles requiring multiple simultaneous interventions; dengue's four serotypes and ADE making vaccination paradoxically risky; partial immunity that doesn't prevent re-infection.
The structural reasons: most burden falls on the world's poorest countries — those least able to fund comprehensive control programs. Remote geography limits access. Climate change expands vector ranges. COVID-19 disrupted delivery systems. No new antibiotic class since 1987; vaccine development takes decades and costs billions.
The lesson: biological innovation alone is not sufficient. A vaccine that works biologically fails if it can't reach people. A tool that reaches people fails if resistance has made it less effective. Solving these diseases requires simultaneous biological innovation and structural investment — which is why malaria, despite having two approved vaccines and effective drugs, still kills a child every two minutes.