Biology • Year 12 • Module 8 • Lesson 19
Visual Disorders, Glasses, Contact Lenses and Eye Surgery
Apply the lesson’s optics and technology framework to real data, patient scenarios, and diagram critique.
1. Interpret the myopia prevalence graph, Australia
The graph below shows the prevalence of myopia (%) in Australian children aged 6–12 years across three decades: 1990, 2007, and 2023. Data are grouped by time spent outdoors each day (less than 1 hour vs 2+ hours). Approximate values are based on trends reported in He et al. (2015, Ophthalmology) and Sherwin et al. (2012, Ophthalmology). 8 marks
Figure 1.1. Myopia prevalence in Australian children aged 6–12 years by survey year and daily outdoor time. Approximate values, after Sherwin et al. (2012) Ophthalmology 119(10) and He et al. (2015) Ophthalmology 122(6).
1.1 Describe the trend in myopia prevalence between 1990 and 2023 for children with less than 1 hour of outdoor time daily. Include figures. 2 marks
1.2 In each survey year, compare the prevalence of myopia between the two groups. What does this suggest about the relationship between outdoor time and myopia? 2 marks
1.3 The lesson states that myopia prevalence is “increasing globally, linked to reduced outdoor time in childhood.” Identify one limitation of using this graph alone to conclude that reduced outdoor time causes myopia. 2 marks
1.4 Predict the corrective technology most likely to be recommended for a 10-year-old child with newly diagnosed myopia of −2.00 dioptres. Justify using the lesson’s evaluation criteria. 2 marks
2. Cause-and-effect chain, how presbyopia develops
Fill in the empty effect boxes to trace the biological pathway from lens ageing to the need for reading glasses. Each arrow indicates a causal step. 5 marks
| Cause: Crystalline lens proteins crosslink and harden with age (from ~mid-40s) | → | Effect 1: The lens loses _____________ and can no longer change _____________ when ciliary muscles contract. | → | Effect 2: The process of _____________ fails, the eye cannot increase its _____________ power for near objects. |
| ↓ |
| Effect 3: Light from near objects, which is more _____________, focuses _____________ the retina rather than on it, near vision is blurred. | → | Overall outcome: A _____________ (converging) reading lens is needed to supply the extra _____________ that the stiff lens can no longer provide. |
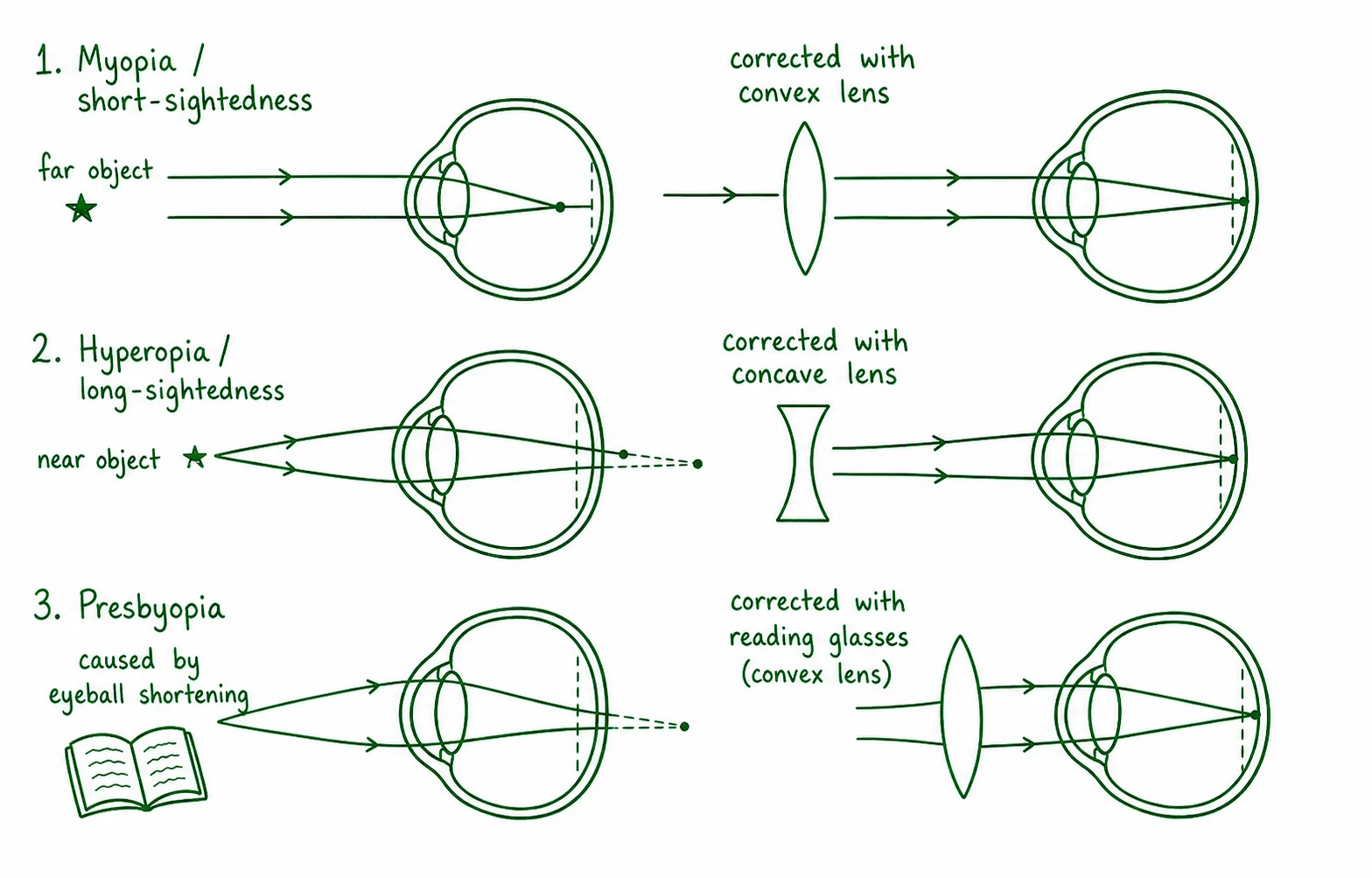
3. Diagram critique, spot the errors in this student’s diagram
A Year 12 student has drawn the diagram below to summarise how glasses correct the three refractive errors. There are three biological errors. Identify and correct each. 6 marks (2 per error: 1 identify, 1 correct)
3.1 Error 1: What is wrong?
Correction:
3.2 Error 2: What is wrong?
Correction:
3.3 Error 3: What is wrong?
Correction:
4. Apply to a patient scenario, Priya’s decision
Priya is a 28-year-old competitive swimmer based in Sydney. She has a stable prescription of +2.00 dioptres (hyperopia) in both eyes and has worn glasses since childhood. She is considering switching to contact lenses or LASIK to improve her performance in the pool. 6 marks
4.1 Explain the anatomical cause of Priya’s hyperopia and describe which type of corrective lens her glasses use and why. 3 marks
4.2 Identify one specific risk of Priya using contact lenses while swimming, and explain the biological basis of that risk. 2 marks
4.3 Predict whether Priya is a suitable LASIK candidate. Identify one eligibility criterion she currently meets and one aspect of LASIK she should understand before proceeding. 1 mark
Q1.1, Trend description
In children with less than 1 hour of outdoor time per day, myopia prevalence increased markedly from 14% in 1990 to 29% in 2007 and then to 52% in 2023, a near-fourfold rise over 33 years. The trend is consistently upward across all three survey years.
Q1.2, Comparison between groups
In every survey year, children with 2+ hours of outdoor time had lower myopia prevalence than those with less than 1 hour (1990: 8% vs 14%; 2007: 13% vs 29%; 2023: 21% vs 52%). This consistent pattern suggests that more time outdoors is associated with reduced risk of myopia in Australian children.
Q1.3, Limitation of graph for causal claim
The graph shows a correlation (association) between outdoor time and myopia prevalence, but cannot establish causation. A confounding variable (e.g. near-work screen time, which is both increasing over time and associated with less outdoor activity) may account for the pattern. Because time outdoors was not experimentally manipulated, reverse causation or another variable could explain the relationship. [Also accept: the data are aggregated; individual exposure was not measured; no control group; ecological study design limitation.]
Q1.4, Technology recommendation
Glasses (spectacles) are the most appropriate technology. At age 10, the prescription is still likely changing, ruling out LASIK (which requires a stable prescription for at least 2 years and is not routinely performed before age 21). Contact lenses carry hygiene compliance risks in children under ~12. A concave −2.00 D glasses lens is safe, reversible, and fully corrective.
Q2, Cause-and-effect chain answers
Effect 1: elasticity / shape. Effect 2: accommodation / refractive. Effect 3: divergent / behind. Overall outcome: convex (converging) / convergence.
Q3, Diagram critique
3.1 Error 1, Myopia corrected with convex lens: The diagram shows a convex (converging) lens for myopia, which is wrong. Myopia already has too much convergence (the focal point is in front of the retina). Adding more convergence would worsen the problem. Correction: Myopia is corrected with a concave (diverging) lens, which spreads light rays and moves the focal point backwards onto the retina.
3.2 Error 2, Hyperopia corrected with concave lens: The diagram shows a concave (diverging) lens for hyperopia. This would move the focal point further behind the retina. Correction: Hyperopia is corrected with a convex (converging) lens, which brings light rays together earlier, moving the focal point forward onto the retina.
3.3 Error 3, Presbyopia caused by eyeball shortening: The diagram states the eyeball shortens with age to cause presbyopia. Correction: Presbyopia is caused by age-related hardening and loss of elasticity of the crystalline lens, not by any change in eyeball length. The eyeball remains normal in axial length; the lens can no longer increase its curvature to accommodate for near objects.
Q4.1, Priya’s hyperopia
Priya’s eyeballs are too short axially, so the focal point for light from near objects would fall behind the retina. Her glasses use a convex (converging, positive power) lens. The convex lens converges incoming light rays before they enter the eye, moving the focal point forward from behind the retina to land on it, allowing both near and distant objects to be seen clearly. [3 marks: 1 for short eyeball/behind retina; 1 for convex lens; 1 for mechanism, converges light to move focal point forward.]
Q4.2, Contact lens risk while swimming
Swimming while wearing contact lenses exposes the lenses to pool water (and natural bodies of water) that may contain Acanthamoeba a microorganism that can cause Acanthamoeba keratitis, a severe corneal infection that can threaten sight. Water also temporarily adheres to lenses, trapping microorganisms against the corneal surface and increasing infection risk. [1 mark for naming the risk, keratitis/infection; 1 mark for biological basis, microbial contamination from water, corneal surface exposure.]
Q4.3, LASIK suitability
Priya meets the key criterion of stable prescription for 2+ years (her prescription has been stable since childhood) and is 28, within the eligible adult age range. She should understand that LASIK is irreversible tissue is permanently removed from the cornea; the correction cannot be undone. She should also understand that LASIK will not prevent presbyopia from developing in her 40s. [1 mark for either: eligible criterion + understanding required.]