Biology • Year 12 • Module 8 • Lesson 17
Prevention, Genetic Disorders, Screening and Gene Therapy
Apply lesson content to real prenatal screening data, inheritance risk calculations, a cause-and-effect mechanism, and an Australian CRISPR case study.
1. Interpret graph, maternal age and trisomy 21 risk
The graph below shows the estimated risk of a live-born infant with Down syndrome (trisomy 21) at different maternal ages, based on Australian and international population data. 8 marks
Data adapted from Hook (1981) Obstetrics & Gynecology 58: 282–285; and Morris et al. (2002) Prenatal Diagnosis 22: 31–39.
1.1 Describe the overall trend in Down syndrome risk with increasing maternal age. Refer to specific data values in your answer. 2 marks
1.2 Estimate the approximate risk per 1000 live births at age 38. Show your reasoning. 1 mark
1.3 Using your knowledge of meiosis, explain the biological mechanism responsible for the steep increase in risk with maternal age. In your answer, refer to non-disjunction and oocyte biology. 3 marks
1.4 Identify which prenatal genetic test, NIPT or amniocentesis, would be most appropriately offered first to a 37-year-old pregnant woman, and justify your choice using information from the lesson. 2 marks
2. Cause-and-effect chain, CFTR mutation to cystic fibrosis symptoms
The boxes below show the cause chain from a CFTR mutation to clinical symptoms of cystic fibrosis. The cause boxes are filled in; complete the effect boxes (shaded). 5 marks
Overall outcome (so…): How does the CF mechanism illustrate why the disease follows an autosomal recessive pattern? 2 marks
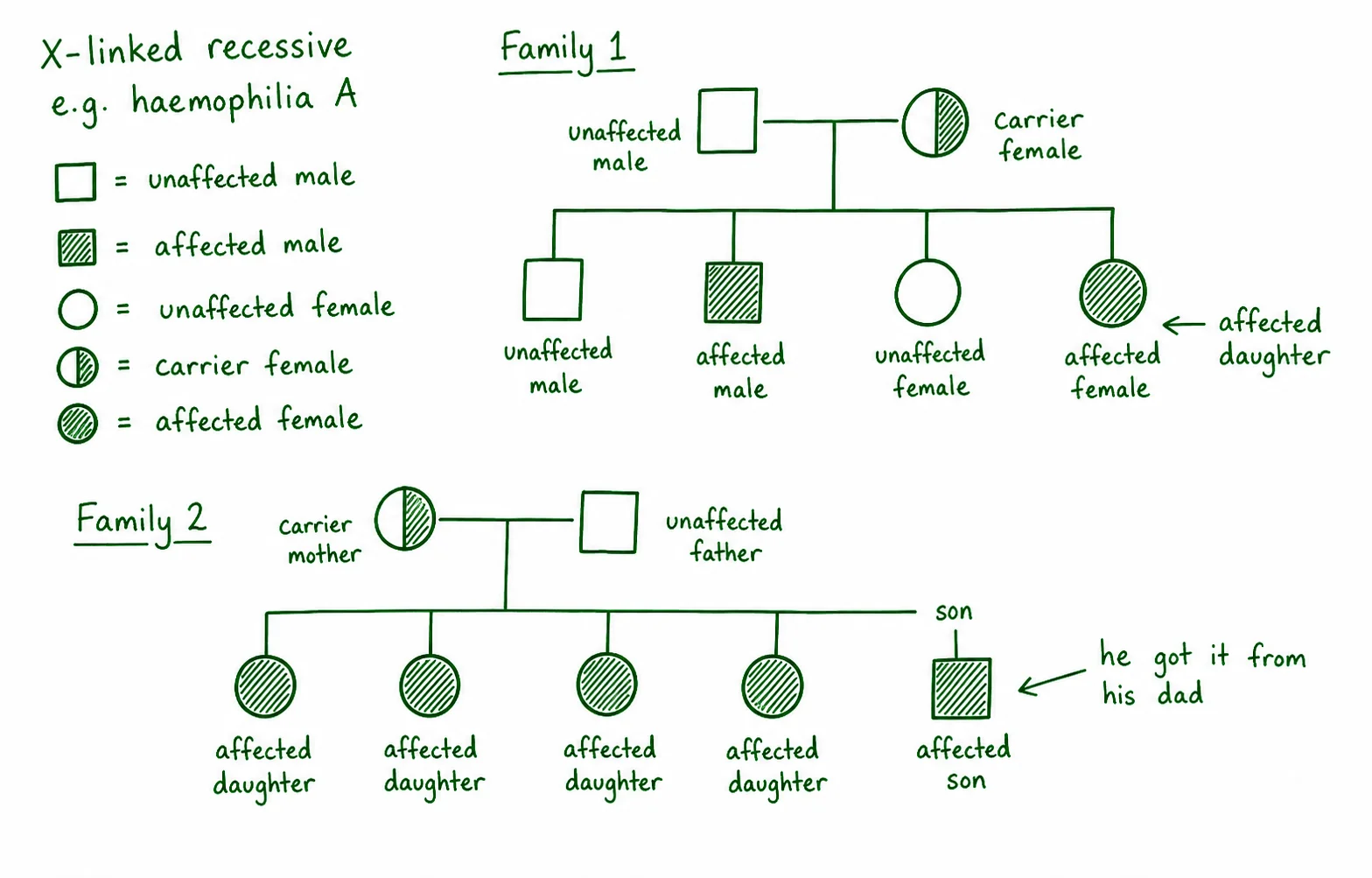
3. Diagram critique, spot the errors in this pedigree
A Year 12 student has drawn a pedigree below and made three biological errors in interpreting an X-linked recessive disorder. Identify each error and write the correction. 6 marks (2 per error: 1 identify, 1 correct)
3.1 Error 1: What is wrong?
Correction:
3.2 Error 2: What is wrong?
Correction:
3.3 Error 3: What is wrong?
Correction:
4. Case study, Casgevy: Australia's first CRISPR treatment access
In November 2023, the US FDA approved Casgevy (exa-cel), the world's first CRISPR-Cas9 therapy, for sickle-cell disease and beta-thalassaemia. The treatment requires harvesting the patient's blood stem cells, editing them with CRISPR to reactivate fetal haemoglobin (HBG1/HBG2 genes), and reinfusing them. The procedure costs approximately AUD $3.5 million per patient. As of 2024, Casgevy is not yet listed on Australia's Pharmaceutical Benefits Scheme (PBS). 6 marks
4.1 Explain why reactivating fetal haemoglobin (HbF) production in a patient with sickle-cell disease is a successful therapeutic strategy. In your answer, refer to: (a) the gene responsible for sickle-cell disease and how the mutation causes the condition, and (b) why fetal haemoglobin can act as a functional replacement. 3 marks
4.2 Explain whether this CRISPR therapy would prevent a patient's children from inheriting sickle-cell disease. Justify your answer with reference to somatic versus germline editing. 2 marks
4.3 Predict and justify one ethical concern raised by the AUD $3.5 million price tag of Casgevy in the Australian health system context. 1 mark
Q1.1, Trend description (2 marks)
The risk of Down syndrome increases with maternal age in a non-linear (approximately exponential) pattern. At age 20 the risk is approximately 0.7 per 1000 live births, rising slowly to 1.1 per 1000 at age 30 [1], then increasing steeply to approximately 10 per 1000 at age 40 and 19 per 1000 at age 45, a roughly 27-fold increase from age 20 to 45 [1].
Q1.2, Estimate at age 38 (1 mark)
Approximately 5–7 per 1000 live births at age 38 (by interpolation between the age 35 value of 2.5 and age 40 value of 10, biased toward 40). Accept any value in the range 4–8 with supporting reasoning. [1]
Q1.3, Biological mechanism (3 marks)
Women are born with all their primary oocytes already arrested at prophase I of meiosis [1]. These oocytes remain in meiotic arrest for decades, at age 40, oocytes have been paused for up to 40 years. During this extended arrest, the molecular structures responsible for chromosomal alignment and segregation (cohesin proteins holding sister chromatids together) degrade [1]. This increases the likelihood that chromosome 21 homologues fail to separate correctly (non-disjunction) when meiosis resumes at ovulation, producing an n+1 egg that gives rise to a trisomy 21 zygote upon fertilisation [1].
Q1.4, Appropriate first test (2 marks)
NIPT should be offered first [1]. It can be performed from 10 weeks gestation, carries no procedural miscarriage risk (non-invasive, analyses cell-free fetal DNA in maternal blood), and is appropriate as a first-line screening tool to identify high-risk pregnancies. If the NIPT result is positive, amniocentesis would then be offered for definitive diagnosis. At age 37 (advanced maternal age), NIPT is commonly offered routinely in Australia [1].
Q2, Cause-and-effect chain
Effect 1: The delta-F508 mutation causes the CFTR protein to misfold; it is recognised by quality-control pathways and destroyed before it reaches the cell surface.
Effect 2: Without functional CFTR in the membrane, chloride ions cannot be transported out of epithelial cells.
Effect 3: Two organs/consequences (any two of): (1) Lungs thick mucus traps bacteria, leading to chronic lung infections (Pseudomonas aeruginosa, Staphylococcus aureus) and progressive lung damage; (2) Pancreas mucus blocks pancreatic ducts, preventing digestive enzymes from reaching the small intestine (malabsorption, failure to thrive); (3) Reproductive tract in males, the vas deferens is blocked by mucus, causing infertility.
Overall (2 marks): CF is autosomal recessive because one functional CFTR allele (in a carrier) produces enough chloride channel protein to prevent the disease phenotype, the single working allele is sufficient for adequate ion transport. Only individuals homozygous for loss-of-function mutations (or compound heterozygotes) produce no functional CFTR and thus develop the disease [1]. This explains carrier status: heterozygous individuals are phenotypically normal but can pass the mutant allele to offspring [1].
Q3, Diagram critique (6 marks)
3.1 Error 1: The mother is labelled "affected" (fully shaded). Correction: A female with haemophilia A must be homozygous XhXh to be affected. A female who has only one Xh allele is a carrier (XHXh), not affected. She should be shown as a half-shaded circle (carrier symbol). [1+1]
3.2 Error 2: Both daughters are shown as affected (fully shaded). Correction: Daughters of a carrier mother and an unaffected father inherit either XH or Xh from their mother and XH from their father, giving XHXH (normal) or XHXh (carrier). Neither daughter receives XhY, daughters cannot be affected unless their father is also affected. They should be shown as half-shaded (carriers) or unshaded (normal). [1+1]
3.3 Error 3: The caption and diagram incorrectly show the son as unaffected and state that "sons are protected by their Y chromosome." Correction: Males have only one X chromosome; a son who inherits Xh from his carrier mother has no second X to compensate, so he is affected (XhY). The son should be shown as fully shaded and the caption corrected. [1+1]
Q4.1, Fetal haemoglobin strategy (3 marks)
Sickle-cell disease is caused by a mutation in the HBB gene, which encodes a subunit of adult haemoglobin. The mutation produces defective adult haemoglobin that causes red blood cells to malfunction (sickling), damaging tissues and organs [1]. Fetal haemoglobin (HbF), encoded by the HBG1/HBG2 genes, does not carry the defect present in adult haemoglobin and can function as a replacement [1]. Casgevy uses CRISPR-Cas9 to edit the patient's own blood stem cells so they reactivate HbF production; the resulting red blood cells contain functional fetal haemoglobin that compensates for the defective adult haemoglobin, relieving disease symptoms [1].
Q4.2, Heritable effects (2 marks)
No, the therapy would not prevent the patient's children from inheriting sickle-cell disease [1]. Casgevy edits the patient's blood stem cells, somatic cells that do not contribute to gamete formation. The patient's sperm or egg cells still carry the original HBB mutation and would transmit it to offspring at the usual Mendelian probability. Only germline editing (modifying eggs, sperm or embryos) would produce heritable changes, and this is banned in most countries due to ethical and safety concerns about altering future generations [1].
Q4.3, Ethical concern (1 mark)
Any one of: Access equity, at AUD $3.5 million without PBS listing, only extremely wealthy individuals could afford the treatment, creating a two-tiered system where genetics-based illness can be treated for the rich but not for most Australians; OR healthcare resource allocation, the cost of treating one patient could fund a much greater total health benefit if distributed across other interventions. [1]