Biology • Year 12 • Module 8 • Lesson 15
Treatment and Management of Non-infectious Diseases
Apply treatment mechanisms, real cost–effectiveness data, and cause-and-effect reasoning to exam-style scenarios.
1. Interpret cost-effectiveness data, statins, metformin, imatinib and CABG
The bar graph below shows the approximate annual cost (AUD) of four non-infectious disease treatments, comparing the unsubsidised market price with the PBS co-payment available to eligible Australian patients in 2024. Use the graph to answer the questions. 7 marks
Figure 1.1. Approximate annual treatment costs in Australia, 2024. Data adapted from PBS schedule and publicly available cost literature. Note: CABG is a one-time surgery; CABG costs shown as an approximate single-procedure cost comparison. Scale is illustrative.
1.1 Identify the treatment with the greatest difference between unsubsidised cost and the cost to an eligible Australian patient. By approximately how much does the PBS/Medicare reduce this cost? 2 marks
1.2 A patient in a country without an equivalent pharmaceutical subsidy scheme requires imatinib. Using the graph data, explain why the biological effectiveness of imatinib does not guarantee that a patient can access it. 3 marks
1.3 Metformin has very low cost even without PBS subsidy. Suggest one reason why low cost alone does not guarantee that a patient will adhere to this treatment long-term. 2 marks
2. Cause-and-effect chain, how exercise treats Type 2 diabetes
The cause boxes are filled in. Complete the empty effect boxes on the right with the biological consequence of each cause. Finally complete the "Overall outcome" statement. 5 marks
Overall outcome (so...):
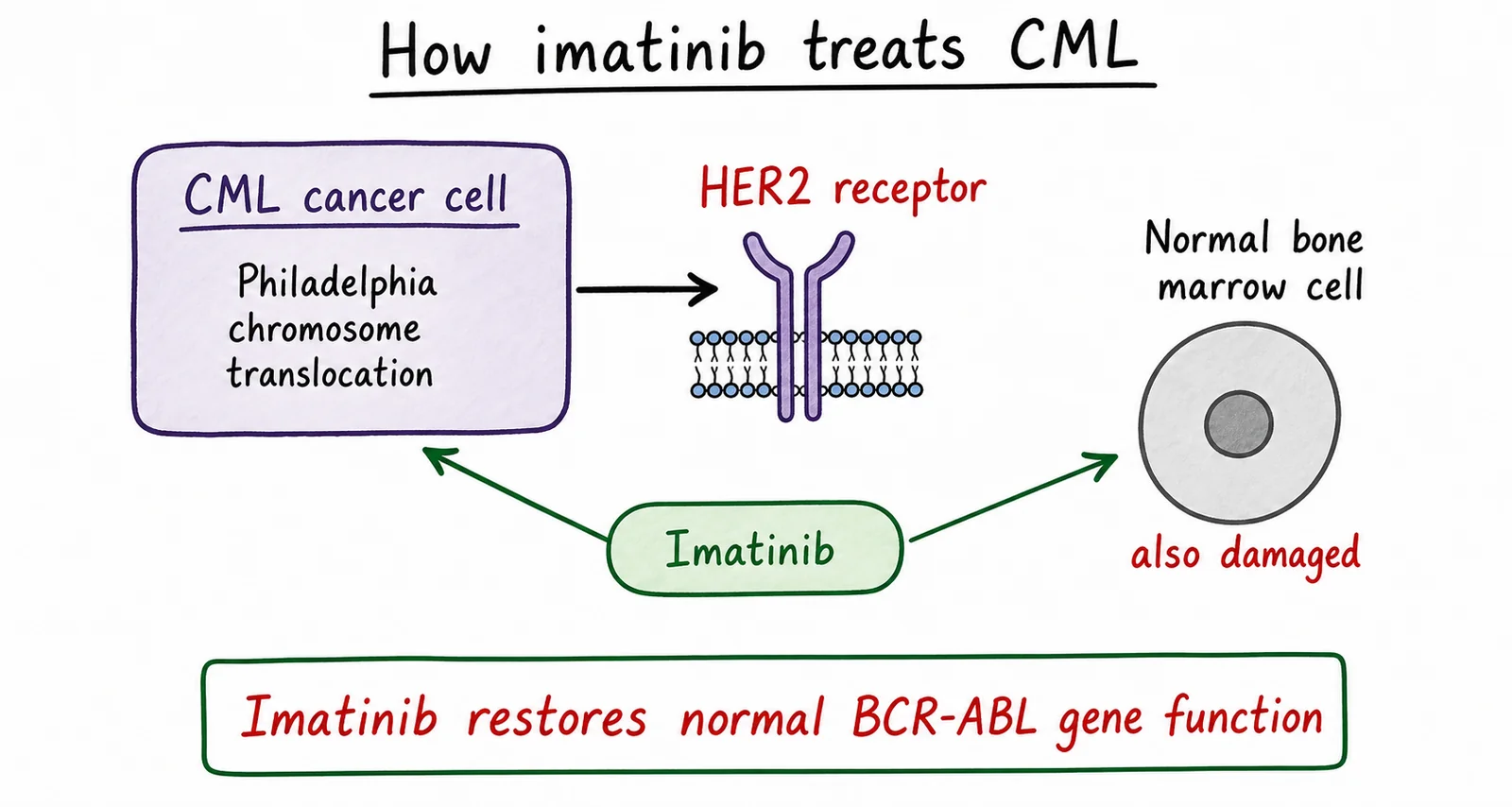
3. Diagram critique, errors in a student's treatment summary diagram
A student has drawn a summary diagram explaining how imatinib treats CML. The diagram contains three biological errors. Identify each error and write the correction below. 6 marks, 2 per error: 1 for identifying, 1 for correcting
3.1 Error 1: What is wrong?
Correction:
3.2 Error 2: What is wrong?
Correction:
3.3 Error 3: What is wrong?
Correction:
4. Case study, Emma's treatment decision
Read the scenario and answer the question below. 5 marks
Scenario. Emma, 52, is a rural Queensland GP who has just been diagnosed with HER2-positive breast cancer (Stage II, no evidence of metastasis). Her oncologist offers two treatment approaches: (A) conventional chemotherapy with cyclophosphamide and docetaxel (a taxane); or (B) trastuzumab (Herceptin), a monoclonal antibody targeted therapy that binds to HER2 receptors on the tumour cells. Trastuzumab is listed on the PBS for HER2-positive breast cancer in Australia. Emma is also told that surgery (lumpectomy) will remove the primary tumour regardless of which pharmacological approach is chosen.
4.1 Using the lesson's framework for evaluating treatments, explain why option (B) trastuzumab is likely to be recommended over option (A) conventional chemotherapy for Emma. In your answer refer to mechanism of action, side effect profile, and at least one factor specific to Emma's circumstances. 5 marks
Q1.1, Greatest PBS/Medicare cost difference
Imatinib (CML) has the greatest difference. The unsubsidised annual cost is approximately $40,000/year; with PBS listing, the annual patient co-payment falls to approximately $480/year, a reduction of approximately $39,500 annually. The CABG procedure is also heavily subsidised, with the full ~$40,000+ surgical cost covered by Medicare for eligible patients.
Q1.2, Biological effectiveness vs access
Imatinib is highly effective at inhibiting BCR-ABL tyrosine kinase in CML cells, achieving 10-year survival rates exceeding 80% [1]. However, without a PBS-equivalent subsidy, the annual cost of approximately $40,000 would require out-of-pocket payment [1]. In lower- and middle-income countries, or systems without pharmaceutical subsidy, this cost is beyond the financial reach of most patients, meaning a biologically effective treatment is inaccessible regardless of its efficacy [1]. Cost and health policy, not clinical effectiveness alone, determine whether a patient can actually receive the treatment.
Q1.3, Low cost ≠ guaranteed adherence
Metformin's initial side effects, including nausea, gastrointestinal discomfort, and diarrhoea, can cause patients to stop taking it before the gut adapts [1]. Low cost does not overcome the barrier of an unpleasant side-effect experience in the early weeks of treatment. Adherence also requires ongoing access to a GP for prescriptions, health literacy to understand why the medication is needed, and motivation to continue a lifelong treatment regimen [1].
Q2, Cause-and-effect chain
Effect 1: AMPK is activated in muscle cells, triggering increased translocation of GLUT4 transporter vesicles to the plasma membrane (independently of insulin receptor signalling).
Effect 2: Glucose is taken up from the blood into muscle cells without requiring insulin, blood glucose concentration falls directly during and after exercise.
Effect 3: Visceral (intra-abdominal) adipose tissue is reduced as the body metabolises stored fat for energy over weeks.
Effect 4: Lower visceral adipose tissue reduces production of adipokines (e.g. TNF-alpha, IL-6) and free fatty acids that impair insulin receptor signalling, insulin sensitivity improves.
Overall outcome: Sustained aerobic exercise and weight loss directly lower blood glucose, improve insulin sensitivity through both GLUT4-mediated uptake and reduced adipokine signalling, and can achieve partial or full T2D remission in early-stage patients without pharmacological treatment.
Q3, Diagram critique
3.1 Error 1 (wrong protein target): The diagram states imatinib blocks HER2 receptor, this is wrong. Imatinib targets BCR-ABL tyrosine kinase, which is produced by the Philadelphia chromosome translocation in CML cells. HER2 is the target of a different drug, trastuzumab (Herceptin), used for HER2-positive breast cancer. Correction: change "HER2" to "BCR-ABL tyrosine kinase" and label it as a CML-specific oncoprotein.
3.2 Error 2 (affects normal cells): The diagram incorrectly shows imatinib damaging normal bone marrow cells. Imatinib's key advantage over conventional chemotherapy is that it only affects cells expressing BCR-ABL, which is exclusive to CML cells carrying the Philadelphia chromosome translocation. Normal cells lack BCR-ABL and are therefore not targeted. Correction: remove the arrow to normal cells and add a note that normal haematopoietic cells are unaffected.
3.3 Error 3 (gene correction claim): The caption "restores normal BCR-ABL gene function" is incorrect, imatinib is a small-molecule kinase inhibitor, not a gene therapy. It does not correct or repair the BCR-ABL gene; it inhibits the abnormal protein product at the molecular level. The gene defect remains. Correction: change caption to "imatinib inhibits the BCR-ABL protein, blocking the proliferative signal in CML cells, the underlying gene abnormality remains."
Q4.1, Emma's treatment decision (5 marks)
Mechanism: Trastuzumab specifically binds to the extracellular domain of HER2 receptors, blocking growth signalling and triggering antibody-dependent immune cell destruction of HER2-positive tumour cells [1]. Cyclophosphamide/docetaxel are cytotoxic agents that disrupt DNA or microtubule assembly in all rapidly dividing cells, not specifically cancer cells [1].
Side effects: Conventional chemotherapy causes immunosuppression (bone marrow suppression), hair loss, severe nausea, fatigue, and infection susceptibility, all of which would impair Emma's capacity to work as a GP. Trastuzumab has a milder side-effect profile with much less bone marrow suppression; cardiac monitoring is required (cardiac toxicity is a known risk) but severe dose-limiting toxicity is less common [1].
Emma-specific factors: Emma is a rural GP, severe chemotherapy side effects (immunosuppression, fatigue) would leave her unable to practise medicine and would significantly reduce her quality of life [1]. Trastuzumab is PBS-listed for HER2-positive breast cancer in Australia, so cost is not a barrier [1]. Because her cancer is localised (Stage II, no metastasis), targeted therapy + surgery offers an evidence-based path to remission with substantially better tolerance.