Biology • Year 12 • Module 8 • Lesson 14
Treatment of Non-infectious Disease
Lock in the core vocabulary, the four treatment categories, and the molecular mechanisms of key therapies, the foundations for applying and evaluating treatment options at HSC level.
1. Term–definition match
The twelve definitions below are shuffled. In the right-hand column write the matching term from this list: pharmacotherapy, curative treatment, symptomatic treatment, lifestyle modification, targeted therapy, palliative care, corrector, potentiator, immune checkpoint inhibitor, statin, ACE inhibitor, antisense oligonucleotide. 12 marks
| # | Definition (shuffled) | Matching term |
|---|---|---|
| 1.1 | Treatment using drugs that target specific molecular or physiological disease mechanisms. | |
| 1.2 | Therapy that eliminates the underlying cause of disease rather than just managing its effects. | |
| 1.3 | Therapy that relieves disease symptoms without addressing the root cause. | |
| 1.4 | Care focused on improving quality of life in serious illness rather than achieving cure. | |
| 1.5 | Changes to diet, exercise, smoking, or other behaviours that directly address the physiological cause of a disease. | |
| 1.6 | Treatment designed to act on a specific molecular target such as a mutant protein or oncogene product. | |
| 1.7 | A drug class that inhibits HMG-CoA reductase in the liver, reducing hepatic cholesterol synthesis and lowering blood LDL. | |
| 1.8 | A drug class that blocks angiotensin-converting enzyme, reducing angiotensin II production and lowering blood pressure. | |
| 1.9 | A CFTR modulator component that helps the misfolded F508del CFTR protein fold correctly so it can reach the cell membrane. | |
| 1.10 | A CFTR modulator component that increases the probability and duration of the CFTR channel being in its open state. | |
| 1.11 | A monoclonal antibody (e.g. pembrolizumab) that blocks the PD-1/PD-L1 pathway to restore cytotoxic T cell activity against cancer cells. | |
| 1.12 | A short synthetic DNA/RNA strand that binds target mRNA and triggers its degradation, reducing production of a toxic protein (e.g. mutant huntingtin). |
2. True or false, with correction
For each statement, circle T or F. If the statement is false, write the corrected version on the line provided. 10 marks (1 for T/F, 1 for each correction where needed)
2.1 Statins dissolve existing atherosclerotic plaques in coronary arteries. T / F
2.2 CFTR modulators like Trikafta treat cystic fibrosis by correcting the F508del DNA mutation at the gene level. T / F
2.3 Cytotoxic chemotherapy kills cancer cells specifically while sparing all normal dividing cells. T / F
2.4 Significant weight loss can achieve Type 2 diabetes remission by reducing visceral fat and restoring insulin receptor sensitivity. T / F
2.5 Immune checkpoint inhibitors like pembrolizumab work by generally boosting all aspects of the immune system simultaneously. T / F
3. Function recall, what does each treatment do?
For each treatment, answer in 1–2 sentences. State the molecular or physiological target and the downstream effect. 10 marks (2 each)
3.1 What is the function of ivacaftor (CFTR potentiator) in treating cystic fibrosis?
3.2 What is the function of atorvastatin in treating cardiovascular disease?
3.3 What is the function of vemurafenib (BRAF inhibitor) in treating melanoma?
3.4 What is the function of ramipril (ACE inhibitor) when prescribed to a patient with hypertension and diabetic nephropathy?
3.5 What is the function of regular moderate-intensity exercise as a treatment for Type 2 diabetes?
4. Fill-in-the-blank, the treatment hierarchy
Complete the passage using words from the word bank below. Each word is used once. 8 marks
Word bank:
symptoms • root cause • mechanism • progression • druggable • CFTR • visceral • remission
Treatments for non-infectious disease can be classified by where they intervene in the disease pathway. The most desirable treatments address the (4.1) _______________________ directly, for example, Trikafta restores the function of the (4.2) _______________________ protein in cystic fibrosis, targeting the protein-level consequence of the F508del mutation. Other treatments act at the (4.3) _______________________ level, interrupting a key step in the disease process without correcting the underlying defect, insulin therapy for Type 1 diabetes is an example. Some treatments slow disease (4.4) _______________________ without stopping it; statins slow atherosclerotic plaque formation by reducing LDL availability. The least-targeted treatments manage (4.5) _______________________ only, without affecting the disease trajectory.
Understanding the molecular mechanism is necessary but not always sufficient to develop an effective treatment, the target also needs to be (4.6) _______________________ by a small molecule or biological agent. In Type 2 diabetes, significant weight loss reduces (4.7) _______________________ adipose tissue, normalises inflammatory adipokine signalling, and can achieve (4.8) _______________________, blood glucose returning to the non-diabetic range without medication.
5. Connect the concepts
Draw labelled arrows between the six terms below to show how they relate to each other. Each arrow must carry a linking phrase (e.g. "inhibits", "restores", "reduces"). Aim for at least 6 labelled arrows. 6 marks
Supplied terms: HMG-CoA reductase • statin • blood LDL • atherosclerosis • cardiovascular disease • LDL receptor.
6. Label the treatment categories diagram
The diagram below shows four treatment approaches and where they intervene in a disease pathway. Write the missing labels into boxes A–H. Draw from the lesson's Card 1 table and Cards 2–4 examples. 8 marks
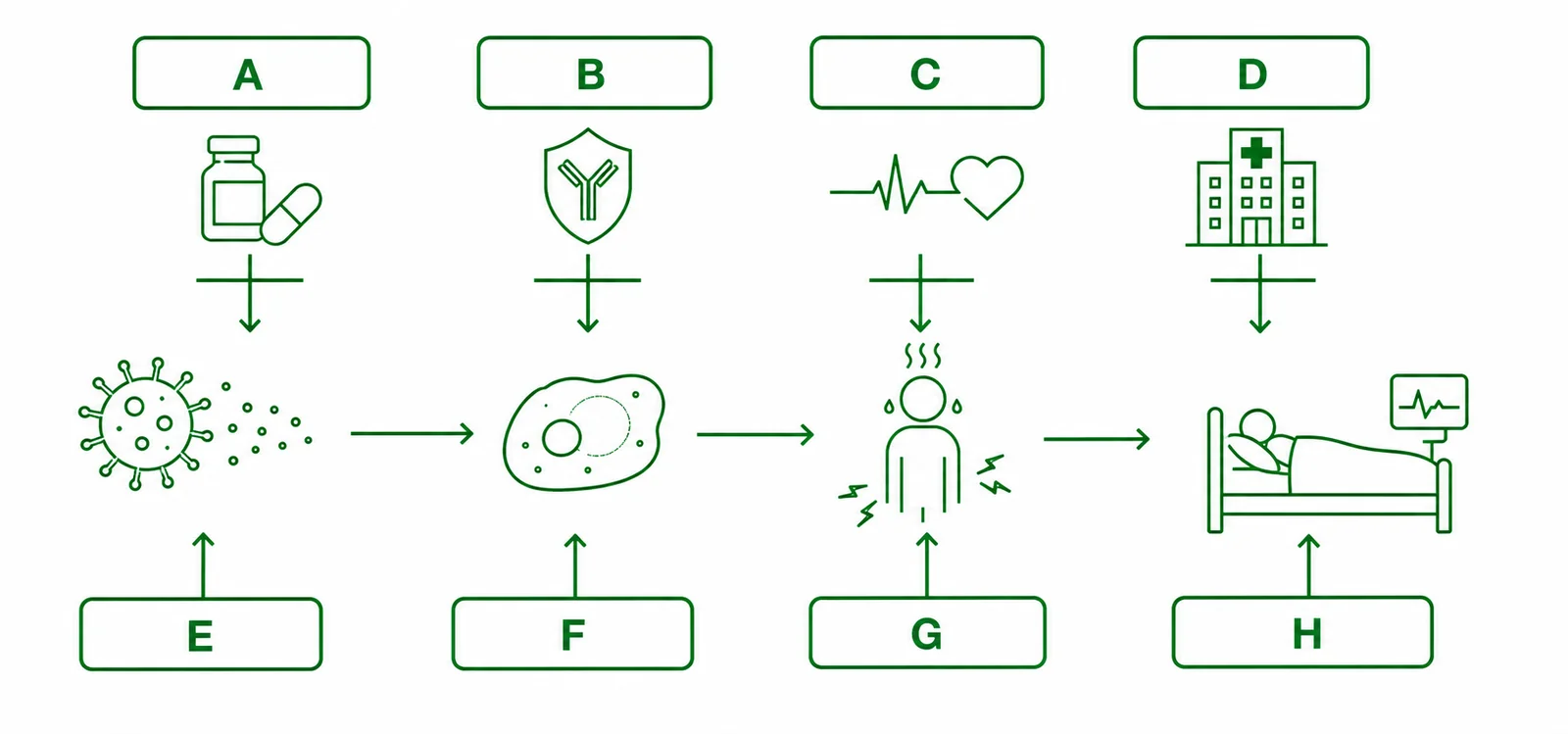
- A, treatment level name (row 1) _______________________
- B, example treatment at level A _______________________
- C, treatment level name (row 2) _______________________
- D, example treatment at level C _______________________
- E, example of a progression-slowing treatment for CVD _______________________
- F, key limitation of progression-slowing treatment _______________________
- G, treatment level name (row 4) _______________________
- H, example treatment at level G for cancer pain _______________________
Q1, Term–definition matches (12 marks)
1.1 pharmacotherapy • 1.2 curative treatment • 1.3 symptomatic treatment • 1.4 palliative care • 1.5 lifestyle modification • 1.6 targeted therapy • 1.7 statin • 1.8 ACE inhibitor • 1.9 corrector • 1.10 potentiator • 1.11 immune checkpoint inhibitor • 1.12 antisense oligonucleotide.
Q2, True / false with corrections (10 marks)
2.1 False. Correction: statins do not dissolve existing atherosclerotic plaques. They inhibit HMG-CoA reductase, reducing hepatic cholesterol synthesis and LDL levels, which slows new plaque formation but does not reverse existing plaques.
2.2 False. Correction: Trikafta does not correct the F508del DNA mutation. The corrector components (elexacaftor, tezacaftor) help the misfolded F508del CFTR protein fold correctly and reach the epithelial cell membrane; the potentiator (ivacaftor) holds the channel open longer. The underlying gene mutation remains unchanged in every cell.
2.3 False. Correction: cytotoxic chemotherapy kills all rapidly dividing cells, cancer cells and normal dividing cells (such as hair follicle cells, bone marrow progenitors, and gut epithelium), which causes the characteristic side effects of hair loss, nausea, and immunosuppression. Targeted therapy (e.g. BRAF inhibitors) is designed to selectively kill cancer cells carrying a specific mutation.
2.4 True.
2.5 False. Correction: immune checkpoint inhibitors like pembrolizumab block the specific PD-1/PD-L1 interaction that cancer cells exploit to switch off cytotoxic T cells. This releases a specific inhibitory brake on T cell activity, it does not generally stimulate all aspects of the immune system, and it can cause autoimmune side effects from disinhibiting T cells in normal tissues.
Q3, Function recall (10 marks, 2 each)
3.1 Ivacaftor (potentiator): Ivacaftor binds to the CFTR chloride channel protein and increases the probability and duration of the channel being in its open state, allowing more Cl− ions to flow into the airway lumen. Water follows by osmosis, hydrating the mucus and restoring mucociliary clearance.
3.2 Atorvastatin (statin): Atorvastatin inhibits HMG-CoA reductase, the rate-limiting enzyme in hepatic cholesterol synthesis. Reduced hepatic cholesterol production causes the liver to upregulate LDL receptors, clearing more LDL from the blood. Lower blood LDL reduces the substrate available for atherosclerotic plaque formation, slowing cardiovascular disease progression.
3.3 Vemurafenib (BRAF inhibitor): Vemurafenib specifically binds and inhibits the mutant BRAF V600E kinase found in ~50% of melanomas. This blocks the constitutive proliferation signal the mutant protein generates, selectively killing BRAF V600E-mutant melanoma cells while sparing normal cells that carry regulated (non-mutant) BRAF.
3.4 Ramipril (ACE inhibitor): Ramipril blocks angiotensin-converting enzyme, preventing formation of angiotensin II. Lower angiotensin II reduces vasoconstriction (lowering blood pressure) and specifically dilates the efferent arteriole of the glomerulus, reducing intraglomerular pressure and slowing the progression of diabetic nephropathy (glomerulosclerosis and proteinuria).
3.5 Moderate exercise: Regular moderate-intensity exercise upregulates GLUT4 transporters in skeletal muscle cells via an insulin-independent pathway (muscle contraction directly stimulates GLUT4 translocation), improving glucose uptake from the blood. It also reduces cardiovascular risk, lowers blood pressure, and improves lipid profile, acting on multiple mechanisms simultaneously.
Q4, Cloze (8 marks, 1 each)
4.1 root cause • 4.2 CFTR • 4.3 mechanism • 4.4 progression • 4.5 symptoms • 4.6 druggable • 4.7 visceral • 4.8 remission.
Q5, Sample concept map (6 marks)
Award 1 mark per correctly labelled, directionally accurate arrow. A correct map should include: statininhibits → HMG-CoA reductase; HMG-CoA reductase (blocked), causes liver to upregulate → LDL receptor; LDL receptorclears from blood, reducing → blood LDL; blood LDLreduced levels slow → atherosclerosis; atherosclerosisdrives → cardiovascular disease; statinindirectly reduces rate of → atherosclerosis. Accept any biologically valid linking phrases and equivalent causal relationships.
Q6, Labelled diagram (8 marks)
A: Root cause (level of intervention). B: Trikafta / CFTR modulators (example). C: Mechanism (level of intervention). D: Insulin therapy for T1D / BRAF inhibitor for melanoma (accept either or equivalent). E: Statins (progression-slowing for CVD). F: Disease continues to progress, just more slowly; patient needs ongoing treatment / existing plaques not reversed. G: Symptom management (level of intervention). H: Analgesics / opioids (for cancer pain).