Biology • Year 12 • Module 8 • Lesson 10
Cancer, Cell Cycle, Oncogenes, Tumour Suppressors and Metastasis
Apply cancer biology to real data, clinical scenarios, and a cause-and-effect analysis of the HPV–cervical cancer pathway.
1. Interpret real data, melanoma five-year survival by stage at diagnosis
The bar chart below shows five-year relative survival rates for melanoma in Australia, stratified by stage at diagnosis. Data from the Australian Institute of Health and Welfare (AIHW), Cancer in Australia 2023. 8 marks
Figure 1.1. Five-year relative survival rates for melanoma in Australia by stage at diagnosis. Source: AIHW, Cancer in Australia 2023. Stage IV approximated from published ranges.
1.1 Describe the overall trend in survival rate as stage at diagnosis increases from Stage I to Stage IV. Quote at least two data values from the graph. 2 marks
1.2 Using your knowledge of the metastatic process (five steps from Card 4), explain why Stage IV melanoma has a dramatically lower five-year survival rate than Stage I melanoma. 3 marks
1.3 The lesson identifies BRAF V600E as the most common oncogene mutation in melanoma, present in ∼50% of cases. BRAF inhibitors such as vemurafenib produced dramatic initial responses in patients with metastatic BRAF-mutant melanoma but most patients eventually relapsed. Predict one biological mechanism by which relapse could occur and justify your prediction using cancer biology from the lesson. 3 marks
2. Cause-and-effect chain, HPV E6 protein and the road to cervical cancer
The left column shows a cause. For each cause, fill in the effect. The chain traces how HPV E6 protein progressively disables normal cell cycle control, culminating in cancer. The final box asks for the overall consequence. 6 marks (1 per effect + 1 overall)
| Cause | → | Effect (your answer) |
|---|---|---|
| HPV 16/18 integrates its DNA into the host cell genome and expresses the E6 protein. | → | |
| E6 protein binds to p53 and targets it for ubiquitin-mediated degradation. | → | |
| p53 is absent from the cell. | → | |
| Cells with DNA damage pass through the G1/S checkpoint unchecked and replicate their damaged DNA. | → | |
| Mutations accumulate progressively in critical regulatory genes over time. | → |
Overall consequence (so…): Explain in one sentence why most HPV infections do not result in cervical cancer, even though the E6/E7 mechanism is powerful.
3. Diagram critique, what’s wrong with this student’s cancer diagram?
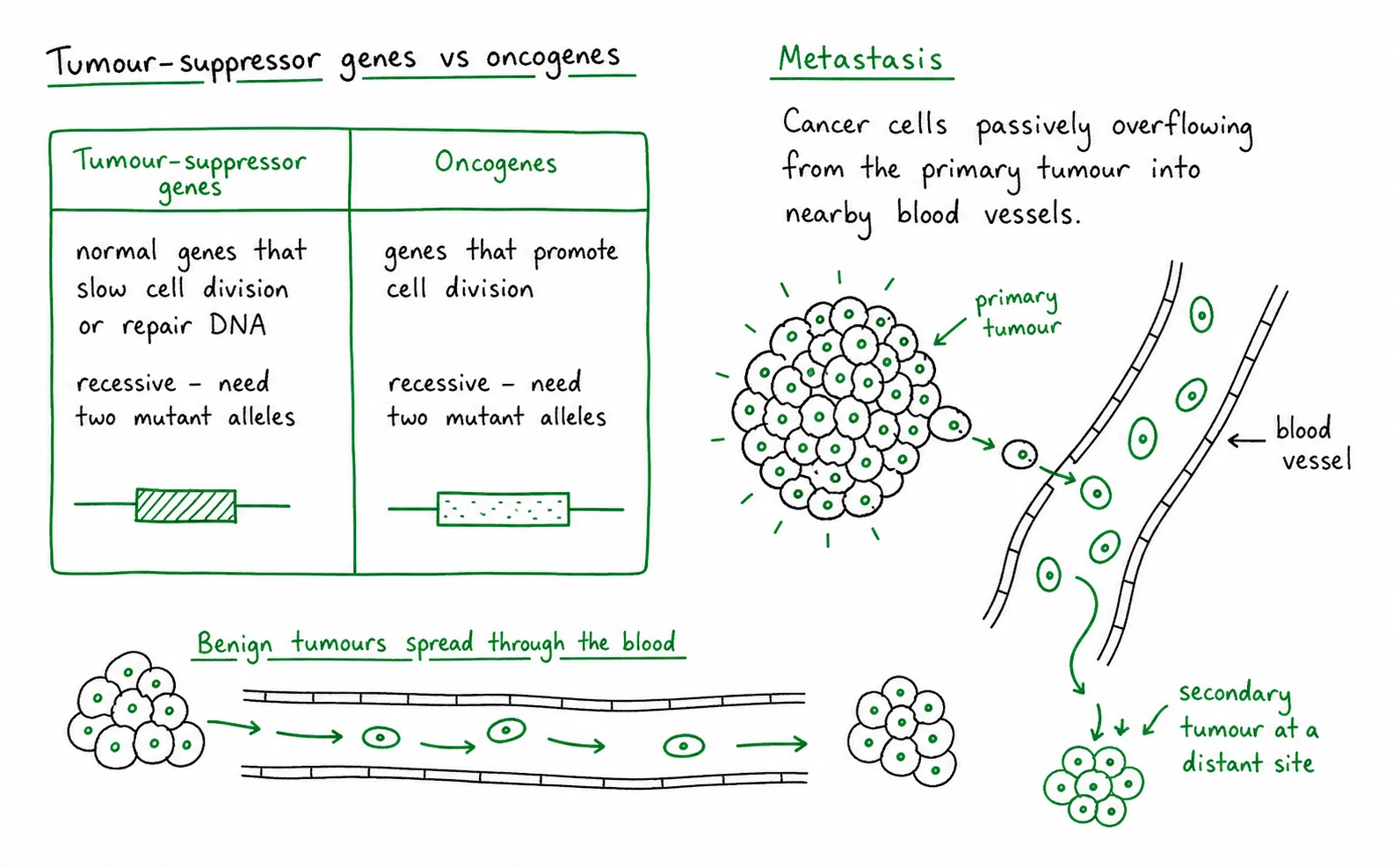
A Year 12 student drew the diagram below to explain metastasis and the tumour suppressor/oncogene distinction. There are three biological errors. Identify each error and write the correction. 6 marks (2 per error: 1 identify, 1 correct)
3.1 Error 1: What is wrong?
Correction:
3.2 Error 2: What is wrong?
Correction:
3.3 Error 3: What is wrong?
Correction:
4. Compare benign and malignant tumours
Complete the comparison table using information from Card 4 of the lesson. 8 marks (1 per completed cell)
| Feature | Benign tumour | Malignant tumour |
|---|---|---|
| Growth pattern | ||
| Tissue invasion | ||
| Metastasis | ||
| Treatment outcome |
Q1.1, Trend description (2 marks)
Five-year survival falls sharply and consistently as stage at diagnosis increases. Stage I yields a survival rate of 99%, near-universal, falling to 68% at Stage II, 47% at Stage III, and only 18% at Stage IV. The difference between Stage I and Stage IV is 81 percentage points, illustrating how dramatically prognosis worsens with advancing disease.
Q1.2, Why Stage IV has lower survival (3 marks)
Stage IV melanoma is metastatic cancer cells have completed all five steps of metastasis (local invasion, intravasation, circulation/survival, extravasation, secondary tumour formation) and established tumours in distant organs [1]. Treatment must now address multiple sites rather than a single localised tumour; surgical excision is no longer curative [1]. Secondary tumours in sites such as the brain, liver, and lungs impair vital organ function, and each secondary tumour may have acquired its own additional mutations, creating genetically heterogeneous disease that responds unpredictably to single-target therapies [1].
Q1.3, Predict a relapse mechanism (3 marks)
A biologically sound prediction: the primary tumour is not genetically uniform, it contains cells with different combinations of mutations (tumour heterogeneity) [1]. A small sub-population of cells may carry a second mutation in the RAS/MAPK pathway (downstream of BRAF) or in BRAF itself (e.g. BRAF splice variant) that bypasses the BRAF V600E inhibition [1]. Because vemurafenib selectively kills BRAF V600E-dependent cells, it removes the “majority” population but acts as a selection pressure enriching for cells that do not require BRAF V600E for proliferation, these cells expand into the relapsed tumour. This is consistent with the lesson’s point that 4–8 driver mutations accumulate progressively; drug resistance is itself a form of clonal selection [1].
Q2, Cause-and-effect chain (HPV E6)
Effect 1: E6 protein is produced inside the infected host cell. Effect 2: p53 protein is degraded / destroyed (ubiquitin-mediated proteolysis). Effect 3: The G1/S DNA-damage checkpoint fails, cells with damaged DNA can no longer be arrested or directed toward apoptosis. Effect 4: Mutations in critical regulatory genes (e.g. TP53 itself, CDKN2A, other tumour suppressors) are copied into daughter cells rather than eliminated. Effect 5: The cell accumulates the 4–8 driver mutations required for fully malignant cervical cancer.
Overall consequence: Most HPV infections are cleared by the immune system before persistent infection can accumulate the additional somatic mutations required for cancer; only persistently infected cells in immunosuppressed or genetically susceptible individuals progress to cervical cancer over years to decades, because cancer requires far more than E6/E7 alone to develop.
Q3, Diagram critique (6 marks)
3.1 Error 1 (oncogenes labelled recessive): Oncogene mutations are dominant, not recessive, one mutant allele is sufficient because the constitutively active protein drives division regardless of the normal allele. Correction: relabel “Oncogenes: dominant gain-of-function, one mutant allele sufficient.” [1 + 1]
3.2 Error 2 (benign tumour spreads through blood): Benign tumours do not invade surrounding tissue or metastasise via blood or lymph, this is the defining feature that distinguishes them from malignant tumours. Correction: “Benign tumours remain localised and do not metastasise; only malignant tumours spread via blood/lymph.” [1 + 1]
3.3 Error 3 (metastasis = passive overflow): Metastasis is not passive overflow due to tumour size. It is an active multi-step process requiring specific additional mutations enabling detachment (loss of E-cadherin, MMP production), survival in circulation (anoikis resistance), and colonisation of distant tissue (angiogenesis). A very large benign tumour never metastasises regardless of size. Correction: “Metastasis requires active molecular machinery: specific mutations in cell adhesion molecules, matrix metalloproteinases, and anoikis resistance pathways.” [1 + 1]
Q4, Benign vs malignant comparison
Growth pattern, Benign: Slow, well-defined, often encapsulated. Malignant: Rapid, irregular, infiltrating.
Tissue invasion, Benign: No, remains localised within its boundary. Malignant: Yes, invades surrounding tissue through degradation of ECM.
Metastasis, Benign: No, does not spread to distant sites. Malignant: Yes, can spread via blood or lymph to establish secondary tumours.
Treatment outcome, Benign: Surgical removal usually curative. Malignant: May require surgery, chemotherapy, radiation, targeted therapy; metastatic disease rarely curable.