Biology • Year 12 • Module 7 • Lesson 16
Antibiotics and Antivirals
Apply mechanisms of antibiotic/antiviral action to real Australian resistance data, a cause-and-effect chain, a resistance trend graph, and a spot-the-error diagram.
1. Interpret Australian Staphylococcus aureus resistance data
The table below shows the percentage of Staphylococcus aureus clinical isolates from Australian hospitals that were resistant to three antibiotics at various years. Use the data and your lesson knowledge to answer the questions below. 10 marks
| Year | Penicillin resistance (%) | Methicillin/oxacillin resistance (MRSA, %) | Vancomycin resistance (%) |
|---|---|---|---|
| 1945 | 0 | N/A (not yet introduced) | 0 |
| 1950 | 40 | 0 | 0 |
| 1960 | 80 | 2 | 0 |
| 1975 | 90 | 15 | 0 |
| 1990 | 95 | 30 | 0 |
| 2005 | 96 | 42 | 0.1 |
| 2020 | 97 | 28 | 0.3 |
Adapted from Australian antimicrobial resistance surveillance data. Methicillin introduced clinically in 1960 as a penicillin-resistant replacement.
1.1 Describe the trend in penicillin resistance from 1945 to 2020. At approximately what point did the rate of increase slow? 2 marks
1.2 Methicillin was introduced in 1960. Using the concepts of natural selection and selection pressure, explain the rise in methicillin resistance between 1960 and 1990. 3 marks
1.3 Methicillin resistance declined slightly from 42% (2005) to 28% (2020). Propose one biological and one public health explanation for this decline. 2 marks
1.4 Vancomycin resistance remained at 0% until after 2000, despite vancomycin being used since the 1950s. Suggest one reason why vancomycin resistance was so much slower to emerge than penicillin resistance. 1 mark
1.5 A hospital pharmacist argues that vancomycin should be reserved as a "last resort" antibiotic. Use the data to justify this strategy. 2 marks
2. Cause-and-effect chain — what happens when you stop antibiotics early
Complete the cause-and-effect chain below. Each cause box is filled; write the effect in the blank box to its right. Then write the overall outcome at the bottom. 5 marks
3. Interpret the antibiotic resistance trend graph
The graph below shows the estimated number of deaths attributed directly to antimicrobial resistance (AMR) globally from 2000 to 2019. 6 marks
3.1 Describe the overall trend in AMR-attributed deaths from 2000 to 2019, quoting at least two data values. 2 marks
3.2 Identify two human behaviours (drawing on lesson content) that are driving this upward trend. 2 marks
3.3 In 2019, AMR directly caused more deaths globally than HIV/AIDS (~860,000) or malaria (~640,000). What does this comparison suggest about the priority governments should assign to AMR as a public health issue? 2 marks
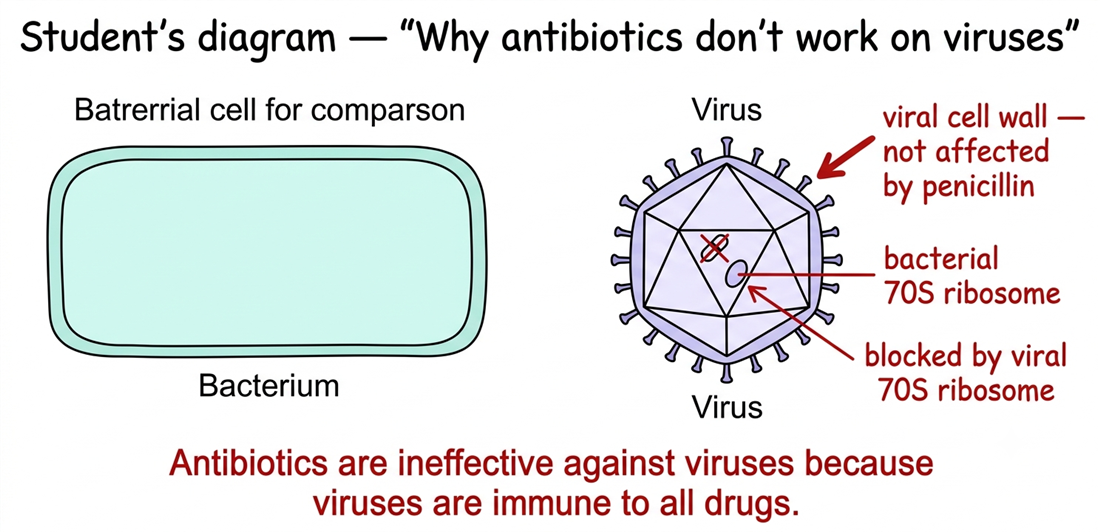
4. Diagram critique — what's wrong with this student's diagram?
A Year 12 student has drawn the diagram below to explain why antibiotics do not work against viral infections. There are three biological errors. Identify each error and write the correction. 6 marks — 2 per error: 1 identify, 1 correct
4.1 Error 1: What is wrong?
Correction:
4.2 Error 2: What is wrong?
Correction:
4.3 Error 3: What is wrong?
Correction:
5. Applied scenario — a GP's prescribing decision
A patient presents to an Australian GP with a sore throat, mild fever and fatigue. A rapid antigen test returns a negative result for Streptococcus pyogenes (the main bacterial cause of severe tonsillitis). The patient asks the GP for amoxicillin (a penicillin-class antibiotic) "just in case". 4 marks
5.1 Give one scientific reason why prescribing amoxicillin in this case would be ineffective. 2 marks
5.2 Give one reason why prescribing amoxicillin could actively cause harm at the community level, even if it causes no direct harm to this individual patient. 2 marks
Q1.1 — Penicillin resistance trend (2 marks)
Penicillin resistance rose sharply from 0% in 1945 to 80% by 1960 [1], then slowed significantly, reaching only 97% by 2020 — the rate of increase levelled off after about 1975–1990, when nearly all susceptible strains in the hospital population had already been eliminated by selection pressure, leaving little further room for percentage increase [1].
Q1.2 — Rise in MRSA using natural selection (3 marks)
When methicillin was introduced in 1960, rare bacterial variants carrying a mutation conferring methicillin resistance (altered penicillin-binding protein, PBP2a) already existed at very low frequency in the S. aureus population [1]. Methicillin acted as a selection pressure: it killed susceptible bacteria while the MRSA variants survived and continued to reproduce [1]. Over successive hospital treatment cycles, the resistant variants became progressively more common as they were not killed and continued to pass their resistance gene to offspring — the classic natural selection mechanism by which the resistant population grew from 2% to 30% [1].
Q1.3 — Decline in MRSA from 2005 to 2020 (2 marks)
Biological: resistant strains often carry a fitness cost (the altered PBP2a is metabolically expensive to produce); in the absence of strong selection pressure, susceptible strains may reproduce slightly faster and regain some frequency in the population [1]. Public health: antibiotic stewardship programs introduced in Australian hospitals from the early 2000s — including restricted prescribing, hand-hygiene campaigns, and isolation of MRSA patients — reduced the transmission of MRSA and the selection pressure driving its spread [1].
Q1.4 — Vancomycin resistance delayed (1 mark)
Accept any one of: (i) Vancomycin was used more restrictively as a last-resort antibiotic, reducing the selection pressure compared to first-line antibiotics used broadly. (ii) Resistance to vancomycin requires multiple complex mutations in cell wall synthesis genes — more difficult to acquire than a single beta-lactamase gene — so resistance was much slower to emerge by chance. (iii) Vancomycin resistance genes are less readily transferred by horizontal gene transfer.
Q1.5 — Justify reserving vancomycin (2 marks)
The data shows vancomycin resistance remained at 0% for decades while it was used less widely, but has begun to appear (0.1–0.3%) since 2005 as MRSA made vancomycin the de facto first-line treatment for many hospital infections [1]. Once vancomycin resistance spreads, there are almost no remaining effective antibiotics for treating MRSA — restricting vancomycin to genuine last-resort use reduces the selection pressure on S. aureus and prolongs the window in which it remains effective, preserving it for patients who truly need it [1].
Q2 — Cause-and-effect chain (5 marks)
Effect 1: The antibiotic acts as a selection pressure — it kills the susceptible majority and reduces the total bacterial population, but the small number of resistant variants survive because the antibiotic cannot eliminate them.
Effect 2: The antibiotic treatment is discontinued prematurely — the remaining bacterial population, now largely composed of the more resistant survivors, is no longer under antibiotic selection pressure.
Effect 3: The surviving bacteria, which are enriched for resistance genes relative to the original population, are free to multiply again without being killed.
Effect 4: The bacterial population rebounds and is now dominated by resistant individuals, as each division passes the resistance gene to daughter cells.
Overall outcome: The infection returns, but the bacterial population is now predominantly resistant to the antibiotic that was originally prescribed — the same antibiotic will be substantially less effective if the course is restarted, and a stronger or different antibiotic may be required.
Q3.1 — Trend description (2 marks)
AMR-attributed deaths rose steadily from approximately 700,000 in 2000 to approximately 1.27 million in 2019 [1], representing an increase of roughly 81% over 19 years, with a consistent upward trend across the entire period and a notably steeper rise between 2015 and 2019 [1].
Q3.2 — Human behaviours driving the trend (2 marks)
Accept any two from: overprescribing of antibiotics for viral infections where they have no effect (creates selection pressure without therapeutic benefit); patients stopping antibiotic courses early allowing resistant survivors to repopulate; agricultural use of antibiotics as growth promoters in livestock at sub-therapeutic concentrations selecting for resistant bacteria in large bacterial populations; self-medication and sharing of antibiotics without medical supervision.
Q3.3 — Comparison with HIV/AIDS and malaria (2 marks)
The data suggests AMR is already a larger direct killer than two of the most funded infectious diseases globally, yet historically received far less research investment and public health attention [1]. Governments should treat AMR as a top-tier global health priority, investing in new antibiotic development, antibiotic stewardship programs, and international coordination to restrict inappropriate prescribing — because inaction allows the death toll to continue climbing, and resistant infections will become untreatable [1]. Accept any response that makes a proportionate argument for elevated government action supported by the comparison data.
Q4 — Diagram critique (6 marks)
4.1 Error 1 ("viral cell wall"): Viruses do not have a cell wall — they consist of a nucleic acid genome enclosed in a protein coat (capsid), not a cell wall made of peptidoglycan or any other polymer. [1 identify] Correction: remove the "viral cell wall" label entirely; explain that viruses have no cell wall, which is why penicillin's mechanism of inhibiting peptidoglycan synthesis cannot act on a virus. [1 correct]
4.2 Error 2 ("viral 70S ribosome"): Viruses do not have ribosomes of any kind. Viruses are not cells and carry no ribosomes; they commandeer the host cell's 80S ribosomes to produce viral proteins. [1 identify] Correction: replace the label with a statement that viruses use the host cell's 80S ribosomes (which are not the target of antibiotic ribosome inhibitors). [1 correct]
4.3 Error 3 ("immune to all drugs"): Antibiotics do not work against viruses because the antibiotic targets (cell wall, 70S ribosome, DNA gyrase, folate synthesis) are absent in viruses — not because viruses are immune to all drugs. Antivirals do work on viruses by targeting virus-specific enzymes and processes. [1 identify] Correction: antibiotics fail against viruses because the specific structures they target do not exist in viral particles. Antivirals (not antibiotics) are the drug class used to treat viral infections. [1 correct]
Q5.1 — Scientific reason amoxicillin is ineffective (2 marks)
Amoxicillin is a penicillin-class antibiotic that works by inhibiting bacterial cell wall (peptidoglycan) synthesis [1]. The patient's symptoms are most likely viral (rapid antigen test is negative for the main bacterial cause) — viruses have no cell wall, no 70S ribosomes, and no folate synthesis pathway for the antibiotic to target, so amoxicillin cannot interfere with viral replication in any way [1].
Q5.2 — Community-level harm (2 marks)
Prescribing amoxicillin kills susceptible bacteria in the patient's gut microbiome without any benefit against the viral infection, creating selection pressure that favours resistant bacteria within the patient's normal flora [1]. This enriches for resistant strains that can subsequently be transmitted to other people in the community — contributing to the broader rise in community-acquired antibiotic resistance even though it did not harm this patient directly. Approximately 30% of antibiotics prescribed in Australian primary care are already considered inappropriate; each unnecessary prescription adds to community-level resistance pressure [1].