Biology • Year 12 • Module 7 • Lesson 1
What Is Infectious Disease?
Apply pathogen classification and disease-transmission concepts to real Australian outbreak data, a case study scenario, and a diagram critique.
1. Interpret outbreak data — COVID-19 transmission settings (Australia, March–May 2020)
The bar chart below shows the proportion of confirmed COVID-19 cases attributed to each transmission setting during the first wave in Australia, based on contact tracing data. 7 marks
Adapted from Australian Government Department of Health COVID-19 Epidemiology Report, April 2020. Contact tracing primary data; setting classified from interview records.
1.1 Identify the transmission setting responsible for the greatest proportion of cases. Suggest one biological or social reason why this setting showed the highest transmission rate. 2 marks
1.2 Classify the contact tracing data represented in this chart as either primary or secondary data. Justify your answer using the lesson's definition. 2 marks
1.3 The "community (unknown source)" category accounts for 19% of cases. Explain what this limitation suggests about contact tracing as a method for collecting complete transmission data. 2 marks
1.4 Identify one additional data collection method that could have provided information about the "community (unknown source)" cases. State what information it would provide. 1 mark
2. Case study — Plasmodium falciparum and malaria in northern Australia
Read the scenario and answer the questions that follow. 6 marks
Plasmodium falciparum is a protozoan transmitted to humans through the bite of female Anopheles mosquitoes. In northern Queensland, health authorities detected a small cluster of locally acquired malaria cases in 2023 — the first such cluster in mainland Australia in decades. Epidemiologists responded immediately, using contact tracing to identify each patient's location on the days before symptom onset, and deploying mosquito traps to collect and test specimens. They also analysed the prior five years of malaria case-reporting data to identify whether any cases had been locally acquired in that period. Both field teams and published disease surveillance records were used in the investigation.
2.1 Classify Plasmodium falciparum into the correct pathogen category and sub-category. Justify your answer with reference to its biological characteristics. 2 marks
2.2 Identify the vector in this scenario. Explain the role of the vector in distinguishing this disease from a non-infectious disease. 2 marks
2.3 Identify one primary data collection method and one secondary data collection method used in this investigation. Explain what each reveals about transmission. 2 marks
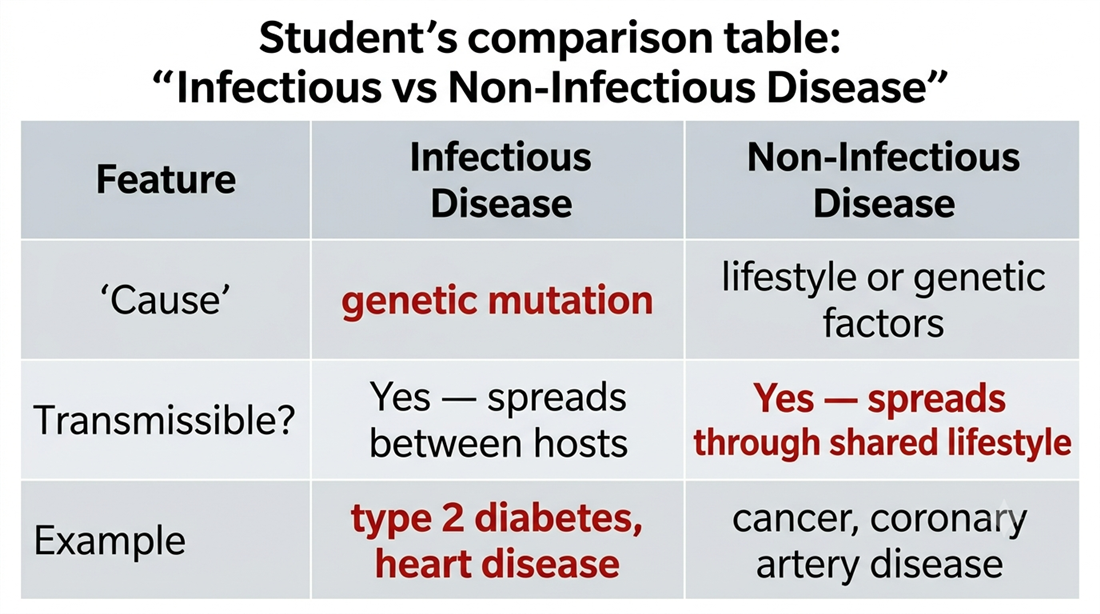
3. Diagram critique — what's wrong with this student's table?
A student has constructed the comparison table below to distinguish infectious from non-infectious disease. There are three biological errors in the table. Identify each error and write the correction. 6 marks (2 per error: 1 identify, 1 correct)
3.1 Error 1: What is wrong?
Correction:
3.2 Error 2: What is wrong?
Correction:
3.3 Error 3: What is wrong?
Correction:
4. Cause-and-effect chain — why pathogen classification determines treatment
Fill in the empty effect boxes to complete the cause-and-effect chain. Each effect follows logically from the cause above it. 5 marks
| A pathogen is classified as a bacterium (a living cell). | → | |
| A pathogen is classified as a virus (non-cellular). | → | |
| A pathogen is classified as a prion (misfolded protein). | → | |
| A pathogen is classified as a fungus (eukaryotic cell). | → | |
| Overall outcome: Correct pathogen classification directly determines the treatment approach and its likely effectiveness. | ||
Q1.1 — Greatest transmission setting + reason
Household contact (38%). Reason: members of the same household share a living space, frequently interact at close range (increasing droplet or contact exposure), and cannot easily maintain physical distance — making sustained, repeated exposure likely before the pathogen is identified and isolation implemented.
Q1.2 — Primary or secondary data?
Primary data. Contact tracing involves epidemiologists directly interviewing diagnosed patients to identify people they encountered during their infectious period. This is data collected first-hand by the investigator, not sourced from records compiled by someone else.
Q1.3 — Limitation of contact tracing (community unknown source)
Contact tracing can only identify transmission events if the patient can recall and name the people they encountered. In community settings — brief encounters on public transport, in shops, or at outdoor events — contacts are often anonymous or forgotten. The 19% "community unknown" category shows that contact tracing is incomplete when transmission occurs through transient, anonymous interactions; these chains cannot be reconstructed from interview data alone.
Q1.4 — Additional data collection method
Serology surveys: testing a population sample for COVID-19 antibodies to estimate how many people have been infected, including those who were not diagnosed or who had no identified contact. This provides population-level exposure data even where individual transmission chains cannot be reconstructed.
Q2.1 — Pathogen classification of Plasmodium falciparum
Plasmodium falciparum is a microorganism — specifically a protozoan (single-celled eukaryote). It is a living cell capable of carrying out metabolic processes (independently and inside host cells), reproducing, and completing a complex life cycle. Because it is a living cell, it belongs to the microorganism category, not the non-cellular category.
Q2.2 — Vector and its role
The vector is the female Anopheles mosquito. A vector transmits the pathogen from one host to another. This distinguishes malaria from a non-infectious disease: the pathogen (Plasmodium) is actively moved between hosts by the vector, making malaria transmissible — a defining feature of infectious disease that non-infectious diseases (caused by genetic or lifestyle factors, not a pathogen) do not have.
Q2.3 — Primary and secondary data methods
Primary: Contact tracing (interviewing patients to identify their movements) and mosquito trapping/testing — both involve investigators collecting data directly in the field. These reveal where transmission is likely occurring and which mosquito populations carry the pathogen.
Secondary: Analysing the prior five years of published malaria case-reporting data. This reveals whether local transmission had occurred previously, enabling epidemiologists to assess whether this cluster represents a new establishment of the pathogen or an isolated event.
Q3 — Diagram critique (6 marks)
3.1 Error 1 ("Cause" row — Infectious Disease column says "genetic mutation"): Infectious diseases are not caused by genetic mutations — they are caused by pathogens (living organisms or agents that invade a host). Correction: replace "genetic mutation" with "pathogen (e.g. bacterium, virus, fungus, prion)" in the Infectious Disease column.
3.2 Error 2 ("Transmissible?" row — Non-Infectious Disease column says "Yes — spreads through shared lifestyle"): Non-infectious diseases are not transmissible from person to person. A shared lifestyle or diet in a household may produce similar conditions, but the disease itself does not pass between people. Correction: replace with "No — cannot spread between individuals".
3.3 Error 3 ("Example" row — Infectious Disease column lists "type 2 diabetes and heart disease"): Type 2 diabetes and heart disease are non-infectious diseases caused by lifestyle and genetic factors, not pathogens. Correction: replace with examples of infectious diseases such as "COVID-19 (SARS-CoV-2), malaria (Plasmodium falciparum), tuberculosis (Mycobacterium tuberculosis)".
Q4 — Cause-and-effect chain
Bacterium → can be targeted by antibiotics, which disrupt bacterial-specific structures (e.g. cell wall synthesis), killing the pathogen or preventing its reproduction.
Virus → antibiotics have no effect (no cell wall, no bacterial metabolism); antivirals or supportive care must be used; antiviral drugs target viral replication inside host cells.
Prion → no standard sterilisation or drug treatment can reliably inactivate it; prions resist heat, radiation, and most disinfectants because they are misfolded proteins — there is currently no cure for prion diseases.
Fungus → requires antifungal agents (e.g. fluconazole, amphotericin B) that target eukaryotic-specific fungal structures (e.g. ergosterol in the cell membrane); antibiotics are ineffective.